European approval for combination lumacaftor/ivacaftor paediatric cystic fibrosis drug
Posted: 22 January 2019 | European Pharmaceutical Review | No comments yet
A paediatric treatment for 2 to 5 year olds has been approved by the European Commission to treat children with the most common form of cystic fibrosis…

The European Commission has granted approval of the label extension for Orkambi (lumacaftor/ivacaftor) for the treatment of children with cystic fibrosis (CF) aged 2 to 5 years old who have two copies of the F508del mutation, the most common form of the disease.
“Today’s approval by the European Commission brings us one step closer to our goal of bringing treatment to all people living with CF,” said Reshma Kewalramani, Executive Vice President, Global Medicines Development and Medical Affairs and Chief Medical Officer at Vertex Pharmaceuticals. “By treating the underlying cause of disease early, we can potentially modify its course and offer patients the chance of improved outcomes.”
The label update is based on data from a Phase III open-label safety study in 60 patients that showed treatment with lumacaftor/ivacaftor was generally well tolerated for 24 weeks, with a safety profile in these paediatric patients generally consistent with that in patients aged 6 years and older.
Lumacaftor/ivacaftor is already approved in the EU for the treatment of CF in patients aged 6 and older who have two copies of the F508del mutation.
Cystic fibrosis is a rare, life-shortening genetic disease affecting approximately 75,000 people in North America, Europe and Australia. It is caused by a defective or missing CFTR protein resulting from mutations in the CFTR gene. As it is a recessive condition, children must inherit two defective CFTR genes – one from each parent – to have CF. There are approximately 2,000 known mutations in the CFTR gene. Some of these mutations, which can be determined by a genetic test, or genotyping test, lead to CF by creating non-working or too few CFTR proteins at the cell surface. The defective function or absence of CFTR protein results in poor flow of salt and water into and out of the cell in a number of organs. In the lungs, this leads to the build-up of abnormally thick, sticky mucus that can cause chronic lung infections and progressive lung damage in many patients that eventually leads to death. The median age of death is in the mid-to-late 20s.
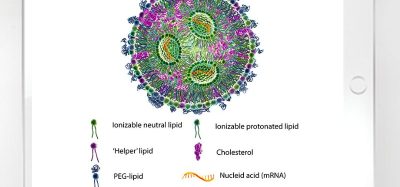
The approved drug is a combination of lumacaftor, which is designed to increase the amount of mature protein at the cell surface by targeting the processing and trafficking defect of the F508del-CFTR protein, and ivacaftor, which is designed to enhance the function of the CFTR protein once it reaches the cell surface.
This European Commission approval is based on a Phase III open-label safety study in 60 patients that showed treatment with lumacaftor/ivacaftor was generally well tolerated for 24 weeks, with a safety profile similar to that in patients aged 6 years and older. Improvements in sweat chloride, a secondary endpoint, were observed at week 24. Researchers also saw changes in key growth parameters, which were also secondary endpoints in the study. The most common adverse event (≥30 percent overall) was cough (63 percent); most adverse events were mild or moderate in severity.
Four patients experienced serious adverse events (two infective pulmonary exacerbations of cystic fibrosis, one gastroenteritis viral, one constipation) and three patients discontinued treatment due to elevated transaminases without concurrent elevations in total bilirubin.
These findings were presented at the 41st European Cystic Fibrosis Society Conference.
Related topics
Clinical Development, Clinical Trials, Drug Development, Research & Development (R&D)