

Converging knowledge and technology to transform neuromuscular disease treatment
Posted: 19 December 2022 | Hannah Balfour (European Pharmaceutical Review) | 1 comment
With the emergence of innovative therapeutic technologies and progress in the genetic understanding of diseases, Biogen’s Toby Ferguson explains why it is a promising time for the development of therapies for neuromuscular conditions such as amyotrophic lateral sclerosis (ALS).
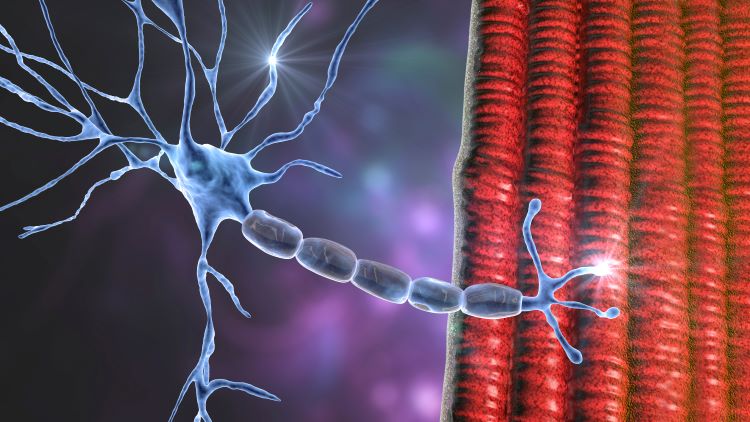
Neuromuscular diseases (NMDs) are a broad group of conditions in which pathologies affect the peripheral nervous system (PNS), the neuromuscular junction or skeletal muscle. NMDs lead to loss of normal nerve and muscle activity and patients lose function. Many NMDs result in atrophy (wasting) of the voluntary muscles.1 The resulting weakness can lead to twitching, cramps, pain, and joint and movement problems. In some cases, heart function and breathing can also be impacted.1 Types of NMD include muscular dystrophies, inflammatory myopathies and motor neurone diseases, such as spinal muscular atrophy (SMA) and amyotrophic lateral sclerosis (ALS) among others.2
There are three approved therapies for ALS in the US and those therapies provide some modest benefit, but patients still have substantial unmet need”
A 2015 epidemiology study looking at 10 prevalent NMDs found most occurred in one to 10 per 100,000 people in the population. At the time, the authors stated that “the sum of the available prevalence rates comprises only the tip of the iceberg,” due to limitations in reporting. They therefore concluded that despite the fact that NMDs are individually considered rare conditions, as a group they were almost as prevalent as Parkinson’s disease.3
ALS is a progressive neurodegenerative disease that affects motor neurons within the brain and spinal cord, resulting in muscle weakness, disability and eventually death. ALS is the most common form of motor neurone disease and reportedly affects between 4.1 and 8.4 per 100,000 people worldwide.4
“There are three approved therapies for ALS in the US and those therapies provide some modest benefit, but patients still have substantial unmet need. In ALS, patients die on average three to five years after diagnosis and that is true for many other neuromuscular diseases as well. In SMA, before the advent of Spinraza and other survival motor neurone (SMN) protein replacement therapies, infants who were diagnosed with the condition often died quite quickly, within the first few years of life. So I think fundamentally the most important reason why neuromuscular disease is an important area for development is that there is a need,” commented Ferguson.
 What are the key challenges for drug developers in the neuromuscular disease field?
What are the key challenges for drug developers in the neuromuscular disease field?
 What are the key challenges for drug developers in the neuromuscular disease field?
What are the key challenges for drug developers in the neuromuscular disease field?Ferguson explained: “Neurology as a field has unmet needs across the board. Simply put, it is difficult. Knowledge of the underlying causes of these diseases is less certain than others and has only emerged in the last few decades. The endpoints – what you need to measure to get a drug approved – are less clear. This recent emergence has made us optimistic but nonetheless, it remains a difficult field.”
In elaborating on the complexity of tackling NMDs, Ferguson stated: “I think what I would highlight as probably the biggest challenge is deciding what aspect of the disease we should try to address in order to make a therapy. The diseases can emerge in any period of life and understanding how they progress and how to measure that progression is always a challenge, as is understanding the underlying biology.”
Having few approved drugs is also a challenge, as the pathway for drug development is less well understood and conversations with regulators are frequently required to decide on appropriate clinical endpoints – something Ferguson claimed was akin to attempting to build a plane while flying it!”
In ALS, for example, he explained that while there are some genetic subtypes, superoxide dismutase type 1 (SOD1) and C9orf72, these account for just 10 percent of patients: “So 90 percent of patients come to the physician, get diagnosed with ALS and we do not understand why the disease has shown up in that person. Therefore, in those people, understanding what biology you need to address to make a drug is very hard. This is a core challenge of many NMDs, and particularly ALS.”
In the clinical development stage Ferguson highlighted two challenges: recruitment and a less well understood development pathway. Recruitment for clinical study is a hurdle because the diseases are so rare: “For instance, SOD1 ALS accounts for approximately two percent of the ALS population worldwide. This translates to approximately 330 patients in the US and a similar number in Europe.” Having few approved drugs is also a challenge, as the pathway for drug development is less well understood and conversations with regulators are frequently required to decide on appropriate clinical endpoints – something Ferguson claimed was akin to attempting to build a plane while flying it!
How has the field developed to overcome these hurdles?
“We have entered a period of time where the types of drugs we can potentially develop and the understanding of genetics, particularly within NMD, can meet these unmet needs for patients,” said Ferguson.
He explained that the convergence of knowledge about NMDs – their causes, pathologies and biomarkers – and clinical development requirements, such as potential clinical endpoints, as well as emerging therapeutic tools is now enabling movement in the space.
What are the key emerging modalities and how is Biogen tackling ALS?
“Fundamentally, it is the modalities that allow you to attack that underlying biology, such as antisense oligonucleotides (ASOs) that allow you to target a particular genetic cause. In SOD1 ALS it is a particular gene to knock down; in Spinraza for SMA ASOs up-regulate splicing at the survival of motor neuron 1 (SMN1) gene. Outside of ASOs, gene therapies are another modality to tackle that underlying genetic cause,” he explained.
Tofersen
Ferguson explained why development programmes have started with the ALS subtypes that have a defined genetic cause, and SOD1 in particular: “One reason for starting with these smaller populations is that we know unequivocally that the cause of the disease in those patients is a mutation in the SOD1 gene. The therapeutic hypothesis is that when the SOD1 gene is mutated the resulting protein is toxic and kills motor neurons, leading to a decline in strength, function and breathing, and the patients’ eventual death – the rate of which is variable. Reducing SOD1 protein should help patients – and that is what we are exploring right now with tofersen.”
Tofersen is an ASO for SOD1 ALS. According to Ferguson, they know from their Phase I and Phase III trials that the ASO successfully knocks down SOD1 by measuring SOD1 protein in the cerebrospinal fluid (CSF).
One reason for starting with these smaller populations is that we know unequivocally that the cause of the disease in those patients is a mutation in the SOD1 gene. “
In Phase I, a dose-finding study, the reduction in the CSF SOD1 concentration between the tofersen groups and the placebo group was dose dependent, with the highest (100mg) dose taken into further development having a difference of -33 percentage points from placebo.5 In Phase III, there were also greater reductions in CSF SOD1 concentration for the 72 participants receiving 100mg tofersen, compared to the 36 on placebo.6
Ferguson commented: “In our Phase I and Phase III VALOR trials there were also substantial reductions of neurofilament, something which has not been demonstrated before to this level in other ALS programmes. Neurofilament is an integral protein found in neurons. In cases of injury or neurodegeneration it is shed into the CSF and blood; with ALS we know neurofilament levels are elevated seven to 10-fold over age-matched controls. These levels also reflect the rate of disease progression; the higher the neurofilament, the more quickly disease progresses and unfortunately the more likely patients will die sooner.”
In Phase I, concentrations of phosphorylated neurofilament-heavy chains and neurofilament‑light chains in blood plasma and CSF were largely unchanged among the 12 participants in the placebo group at day 85, whereas in the 10 participants who received 100mg tofersen the concentrations decreased from baseline.5 In Phase III, there were greater reductions in the concentrations of neurofilament‑light chains in plasma for those on 100mg tofersen versus placebo.6
“The late-stage trials for tofersen had a six‑month placebo control period and then patients were followed for up to 52 weeks. Though we did not meet the six-month primary endpoint, when patients are followed for longer, the patients who were always on the drug did better on measures of ALS function, strength, breathing and multiple patient-reported outcomes, compared to the patients who received the drug only after the first six months on placebo. There also appears to be a potential early survival effect.”
To be successful I would simply say, stick with it. I think that persistence is critical to innovating in the field.”
General ALS
Beyond specific genetic subtypes of ALS, Ferguson also explained that Biogen has a programme for broad ALS in which there is no established genetic target: “The strategy we have taken in broad ALS is to look for underlying genetic signatures we think are important in the disease, even if it is broad.”
In approximately 90 percent of ALS patients, a protein called TDP-43 is found to aggregate and thus is thought to play a pathologic role. Preclinical research suggests Ataxin-2 (ATXN2), a protein in humans encoded by the ATXN2 gene, is an important modulator of TDP-43 pathology – increasing ATXN2 exacerbates motor neuron death while decreasing it limits the toxicity and may improve functionality. Biogen, said Ferguson, is developing an ASO to bind to ATXN2 messenger RNA (mRNA) and mediate its degradation, reducing ATXN2 protein levels and potentially slowing disease progression for the broad ALS population. This programme is currently undergoing Phase I development.
What will be the key to successfully developing transformative treatments for neuromuscular disease such as ALS?
“I am excited and optimistic for the NMD field given the tools we now have. When I was a young resident in neurology, I could not imagine what we have now. For instance, we were taking care of SMA babies and there was no treatment. Now, 15 years later, we have changed the lives of babies with SMA. That is remarkable,” said Ferguson.
“To be successful I would simply say, stick with it. I think that persistence is critical to innovating in the field. This is not a simple disease space; you are trying to learn new things about diseases that have not really been approached by drug developers in the past. So, if you have a failure, keep going. Each time there is a lesson to be learnt,” he concluded.
About the author
Hannah Balfour is the former Science Writer for European Pharmaceutical Review.
 Toby Ferguson, MD, PhD Toby is Vice President and Head of the Neuromuscular Development Unit at Biogen. He is a neuromuscular neurologist and neuroscientist whose professional experience has been focused on developing treatment for neuromuscular disease. Toby plays a key role in developing ALS clinical trials, and in driving preclinical strategy within neurodegenerative and neuromuscular diseases. Toby trained in neurology and neuromuscular disease at the University of Pennsylvania and obtained an M.D. and Ph.D. (Neuroscience) at the University of Florida; he maintains an interest in axon regeneration and degeneration.
Toby Ferguson, MD, PhD Toby is Vice President and Head of the Neuromuscular Development Unit at Biogen. He is a neuromuscular neurologist and neuroscientist whose professional experience has been focused on developing treatment for neuromuscular disease. Toby plays a key role in developing ALS clinical trials, and in driving preclinical strategy within neurodegenerative and neuromuscular diseases. Toby trained in neurology and neuromuscular disease at the University of Pennsylvania and obtained an M.D. and Ph.D. (Neuroscience) at the University of Florida; he maintains an interest in axon regeneration and degeneration.
References
- Neuromuscular disorders: Neuroscience nursing: Royal College of Nursing [Internet]. The Royal College of Nursing. [cited 2022Sep]. Available from: https://www.rcn.org.uk/clinical-topics/Neuroscience-nursing/Neuromuscular-disorders
- Find a neuromuscular disease [Internet]. Muscular Dystrophy Association. 2020 [cited 2022Sep]. Available from: https://www.mda.org/disease/list
- Deenen JCW, Horlings CGC, Verschuuren JJGM, et al. The epidemiology of Neuromuscular Disorders: A comprehensive overview of the literature. Journal of Neuromuscular Diseases. 2015;2(1):73–85.
- Longinetti E, Fang F. Epidemiology of Amyotrophic Lateral sclerosis: An update of recent literature. Current Opinion in Neurology. 2019Oct;32(5):771–6.
- Miller T, Cudkowicz M, Shaw PJ, et al. Phase 1–2 trial of antisense oligonucleotide tofersen for sod1 ALS. New England Journal of Medicine. 2020Jul9;383(2):109–19.
- Miller TM, Cudkowicz ME, Genge A, et al. Trial of antisense oligonucleotide tofersen for sod1 ALS. New England Journal of Medicine. 2022Sep22;387(12):1099–110.
This article originally featured in European Pharmaceutical Review Issue 6 2022. Subscribe to EPR for free!
Issue
Related topics
Biopharmaceuticals, Drug Development, Research & Development (R&D), Therapeutics
Related organisations
Related people
Related diseases & conditions
amyotrophic lateral sclerosis (ALS), Neurodegenerative diseases, Spinal muscular atrophy (SMA)




Nice article! Thanks for sharing informative post Keep posting