Currently, subcutaneous delivery of therapeutic proteins is a fast-growing field, especially for such established modalities as monoclonal antibodies, which require large quantities of drug to be administrated. Different approaches, including high protein concentration, speciality formulations and drug delivery matrices, as well as devices enabling a more rapid administration of larger liquid volumes, are being developed. The fastest growing field is the development of drug-device-combination products, requiring optimisation of highly complex and dynamic systems. The early identification of patients’ needs translated into target product profile for drugs and devices, as well as their integration during the development process, are key success factors. The state of this field will be discussed in this article.
Biopharmaceutical products emerged as a direct consequence of the explosive development of life sciences and, in particular, cell and molecular biology during the past few decades. Biotherapeutics represent a broad range of molecules: hormones, growth factors, peptides, small proteins, cytokines, therapeutic replacement enzymes, blood factors, anticoagulants, monoclonal antibodies, their fragments and fusion proteins, and there are now over 170 launched products1. The first approved biopharmaceutical drug product was the hormone recombinant human insulin, marketed by Eli Lilly as Humulin in 1982 and produced by the process developed at Genentech as secreted from the correspondingly started cell culture1.
This webinar showcases the Growth Direct System; an RMM (Rapid Microbial Method) that improves on traditional membrane filtration, delivering increased accuracy, a faster time to result, enhanced data integrity compliance, and more control over the manufacturing process.
Key learning points:
Understand the benefits of full workflow microbiology quality control testing automation in radiopharmaceutical production
Learn about ITM’s implementation journey and considerations when evaluating the technology
Find out how the advanced optics and microcolony detection capabilities of Growth Direct® technology impact time to result (TTR).
Don’t miss your chance to learn from experts in the industry –Register for FREE
In 1995 Genzyme pioneered the concept of enzyme replacement therapy by introducing to the market the recombinant product imiglucerase (Cerezyme), obtained from genetically engineered Chinese hamster ovary cells. In 1997 the first full length chimeric monoclonal antibody, rituximab, and the first full length humanised monoclonal antibody, daclizumab, were approved for commercialisation2,3. This started the era of monoclonal antibody biotherapeutics, currently the fastest growing field of pharmaceuticals with projected annual sales of 125 billion US dollars by 20204 . Presently, the annual sales of Humira (a monoclonal antibody which inhibits TNF to generate antiinflammatory effect) are above 12 billion US dollars4 . Humira (the biggest blockbuster biotherapeutic of today) is a monoclonal antibody drug product that is administered at high concentration in liquid formulation in a prefilled syringe (PFS) for subcutaneous administration. It has set the bar high and paved the way for increasing convenience to patients.
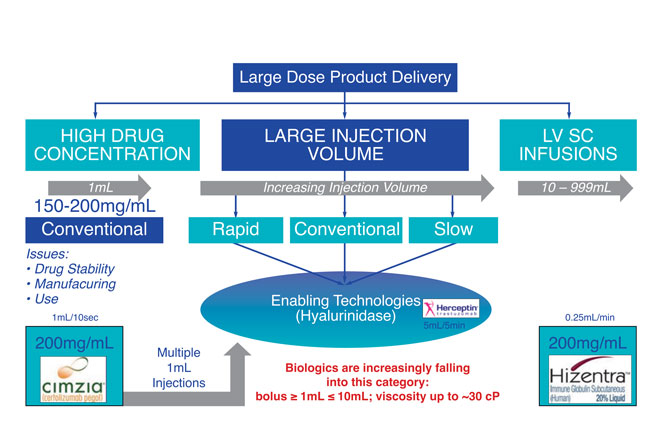
Figure 1: Schematic diagram of the possible routes for large dose product delivery
Formulation approaches
The emergence of biotherapeutic drug products required innovative approaches in process development, including novel approaches in formulation; this is very different from those applied to small-molecule drugs. Biotherapeutics are complex molecules with marginally stable conformational and colloidal stability, so that physical stability (to avoid any fold compromise, potentially leading to particulate matter formation in the size range from aggregates to visible flocculants) and chemical stability (to avoid any hydrolysis, deamidation, oxidation racemisation or isomerisation) are to be optimised during formulation development2. Originally, the main approach to biotherapeutic drug formulation development was lyophilisation, as removal of water significantly slowed chemical degradation processes and improved longterm stability. Lyo formulation development requires optimisation of the vehicle composition followed by lyo cycle optimisation for time-efficient water removal (economic considerations) without compromising potency of the biotherapeutic drug.
Lyophilised formulations enable extended shelf life times, however, they are costly compared with liquid formulations
Lyophilised formulations enable extended shelf life times, however, they are costly compared with liquid formulations, typically requiring additional manufacturing steps, including reconstitution prior to administration and, therefore, are less suitable for in-home administration5,6. Later on, liquid formulation development for biotherapeutics took off and this is currently the most promising approach, especially for monoclonal antibodies5-9, in improving patients’ convenience. Buffers such as histidine, citrate, phosphate, acetate; and tonicifiers such as polysaccharides (trehalose, sucrose, etc.) and polyols (mannitol, sorbitol, etc.) are widely used as vehicle components for monoclonal antibody liquid formulations10.
Non-ionic surfactants, primarily Polysorbates 80 and 20, as well as Poloxamer, became practically universal in both lyo and liquid formulation development, to prevent aggregation and particulate formation10 – the primary physical degradation events for bio therapeutics on freeze thaw and shear stresses. Biotherapeutics formulation development has to operate with a very small number of buffers and tonicifiers due to the limited number of approved excipients for parenteral use. Introduction of novel excipients requires extensive toxicology work and is usually avoided by the biotherapeutics drug development companies11.
Differing potencies
Biotherapeutics vary significantly in their potency, with hormones such as insulin being administered at a very low dose, while monoclonal antibodies require high dose administration. Unlike small molecules, biotherapeutics are currently unsuitable for oral administration, as they get degraded in the gastrointestinal tract. Initially, this class of drugs was primarily targeted for intravenous (IV) administration, and glass vials with rubber stoppers were the predominant container closure sets for the products. The use of subcutaneous (SC) administration for monoclonal antibody parenteral drugs has been restricted by technology, as development of formulations for SC administration is more challenging than that for IV products due to the design space being limited to lower volume dosages of isotonic solutions of highly concentrated drugs. In addition, buffers such as citrate, reported to cause pain at the SC administration site, would be better avoided12. Moreover, SC drug delivery by injection is generally limited to 1-1.5mL, so pre-filled syringes were originally the only container closures for biotherapeutics, designed for SC administration. SC delivery of larger volumes of drug requires a slower rate of administration that is not achievable with a hand-held syringe and needle alone.
Presently, SC administration is becoming increasingly popular in the target product profile and development studies design. From a patient’s perspective, it is less invasive than the IV route and is therefore highly suitable for home-care treatment and self-administration. Commercial biotherapeutic drug products developed in PFS include Enbrel (Amgen), Humira (Abbott/Abbvie), Herceptin (Genentech/Roche) and Simponi (Jannsen/Johnson&Johnson). A schematic diagram of the possible routes for large-dose biologics’ SC drug delivery is presented in Figure 1.
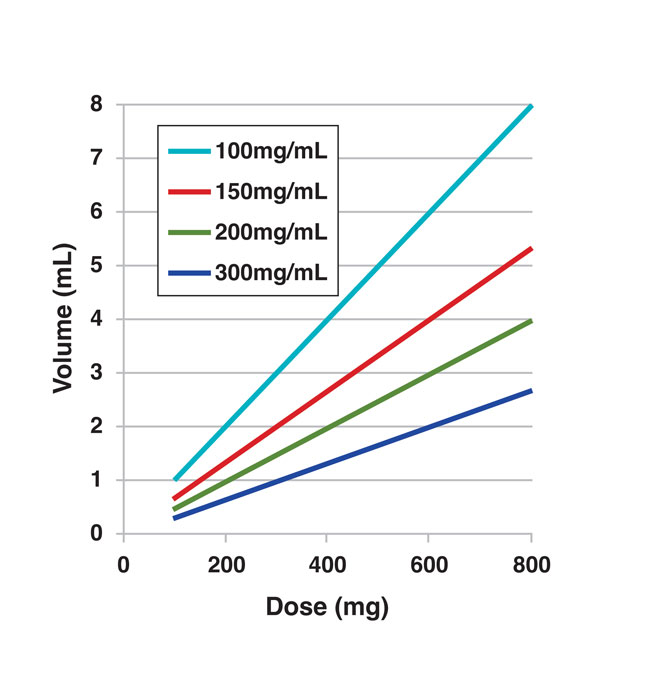
Historically, the first approach was having a high concentration of the drug (up to 200 mg/mL and above) for a 1–1.5 mL volume in a PFS8 . The need for higher concentrated drug formulations, demonstrating the limitation of conventional PFS range for doses above 200-300 mg per injection, is illustrated in Figure 2. A high concentration formulation approach is limited by solubility of the monoclonal antibody as well as by high viscosity of the resultant solutions, often making manufacturing, handling and administration of the products impractical (once viscosity typically exceeds 20-30 cP)8 . Special experimental (analysis of second virial coefficient, diffusion and sedimentation interaction parameters and linkages to viscosity; correlation of zeta potential and an effective isoelectric point with viscosity, to name a few13,14,15) and theoretical (molecular simulations16) tools are being designed. Such tools will be used to evaluate the solubility and manufacturability of the early-stage drug candidates for predictive analysis of the molecule attributes at high concentration to enable engineering of monoclonal antibodies compatible with SC administration17,18.
Different factors, such as molecular shape, size, self-crowding, as well as electrostatic intermolecular interactions, were shown to affect monoclonal antibody viscosity at high concentration19,20. The studies paved the way for rational monoclonal antibody design to disrupt aggregation-prone regions resulting in significant reduction of the solution viscosity at high protein concentrations21. Alternatively, to overcome the viscosity limitations for highly soluble monoclonal antibodies, novel excipients22,23 or non-aqueous suspensions24 as well as novel delivery matrices (silk protein, for instance25,26) are being evaluated. Due to limitations to approved excipients, the current most promising approach involves adding selected amino acids to the composition vehicle, the accumulated empirical data documenting its random efficiency24,27.
Figure 2: Injection volume required for different doses as a result of the drug concentration in formulation
Novel technologies
The growing patient need for autonomous self-administration of biologics drugs in volumes exceeding approximately 1.2mL (conventional PFS range) drives novel technology development. Currently most in demand are boluses within a range between 1mL and 10mL. One approach to overcome the PFS delivery limitation involves Enhanze technology from Halozyme, where co-formulation with recombinant human hyaluronidase enzyme (rHuPH20) enables an increase in injection volume of up to 5mL using PFSs without any significant adverse injections site effects28.
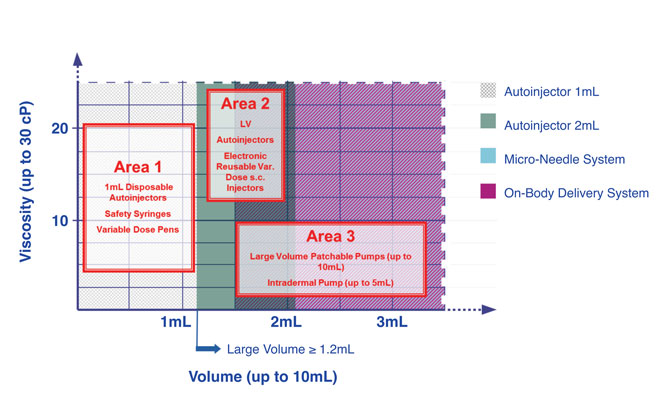
Alternatively, drug delivery devices such as autoinjectors (volumes up to 2mL) or on-body delivery systems enabling slow SC drug delivery (volumes typically up to 5-10 mL), offer new technical solutions for SC delivery of high-concentration biotherapeutics drugs. Figure 3 illustrates current trends in the SC delivery approaches for biologics. The various device systems can typically be grouped into three categories (Figure 3) 29. The cluster of device concepts that exceed delivery volumes of a standard PFS are presented in category two and category three. While category two relies on autoinjectors, including electronic reusable injectors, category three represents typically body-worn pump systems. These manifold delivery systems are emerging on the market with a broad variety of actuator technologies (e.g., mechanical spring, battery and electric motor) and primary container concepts (glass and polymer). The most popular concepts appear to be those that have a preloaded drug container that is irreversibly built-in to the delivery device unit representing drug-device-combination products. Once the drug is emptied from the container the whole system is disposed after use30-32.
Numerous factors, critical for patient acceptance and thus commercial success of such products, are being contemplated: drug formulation (such as pH, osmolality and viscosity), needle gauge, injection speed, injection volume and many subjective factors related to the patient’s experience on drug administration (including pain or discomfort). As a result of this, extensive studies of therapeutic targets and related user groups are required to identify the crucial human factors for particular drug device combination products.
Figure 3: Large volume device landscape
For SC administration, the most significant element for acceptability of administering complete doses (dosing accuracy) is managing discomfort or pain during the treatment33,34,35. One of the earliest investigations of the pain correlation with dose volumes ranging from 0.2-1.5 mL was made by Jorgensen et al. and this study led to further investigations of patient experience with SC administration33. As a response to this trend guidelines stemming from European Union and United States regulatory agencies and associated technical standards (e.g., ISO standard series 11608 [“Needle-based injection systems for medical use – Requirements and test methods”]) have been established34,37. From the drug product development perspective, introduction of novel container closure systems into the practice of biotherapeutics drug delivery devices requires intensive compatibility studies for evaluation of any potential adverse effects of internal surfaces (for instance, siliconisation of PFS38) on the physical stability of the biomolecules. It also limits the list of applicable buffers and excipients (e.g., significant pain on SC administration of citrate has been documented39 but not histidine buffered media).
In addition, extensive extractables and leachables profile analyses are needed to ensure safety of the developed combination products38. These activities are essential to avoid immunogenic and toxicity effects on monoclonal antibody drug delivery using large volume devices. Furthermore, more recent studies focus on the bioavailability of the monoclonal antibodies upon SC delivery40,41. The first developed in vitro model facilitated the establishment of significant variability in bioavailability of the first tested monoclonal antibodies on SC administration, affected by various factors, including formulation components41.
The fact that biotherapeutics are relatively more expensive and more complex to administer drives the demand for tighter therapeutic control by healthcare providers and payers, as well as adherence to therapy instructions by the patients. A technical solution to enable this is to connect the drug delivery device with wireless and electronic devices, such as by combining them with smart phone capabilities32,42. This is a very recent development for which there is presently no clear observable direction.
Although there is an increasing trend to SC large volume delivery driven by the need for an alternative to parenteral delivery of biotherapeutics, as well as the need for a patient-friendly administration as much as possible, those requirements are quite diverse so that there is no single large volume device to be considered a universal technology solution.
Nonetheless, the latest update by MedGizmo (February 2016) claims that 67% of the large-volume wearable injectors (also called bolus injectors) are being operated electronically, with the market for such products being projected to generate 8 billion US dollars in device sales by 202443. With the majority of the developed devices being targeted at volumes below 5mL, some are projected to expand the injectable volume to 30mL. The main area of applicability of these devices is likely to be targeted to self administration or home-care, with up to 50% use being projected for cancer drug delivery.
This is an exciting period in the development of biotherapeutics with novel approaches enabling a dramatic shift to SC drug self-administration with significantly improved patient experience. Due to the steep growth rate of biotherapeutics’ share in the pharmaceutical industry and high competition on the drug market, the enabling innovations described are likely positioned for fast commercial implementation. The future will reveal which of the current technology trends will spawn the most user-friendly and reliable drug delivery systems in the biotherapeutics field.
About the authors
Till Bussemer, PhD, is presently Head of BioFormulation Development at Sanofi in Frankfurt, Germany, and focuses on monoclonal antibodies and large molecules. Dr Bussemer started his career at Aventis Pharmaceutical Development in 2002, where he was responsible for preformulation and formulation of solids and injectables, including depot formulations for species ranging from small molecules to biologics. Recently, Till has also become Drug Device Integrator.
Bernardo Perez-Ramirez, MSc PhD, is currently Senior Scientific Director of BioFormulations in the Biopharmaceuticals Development department of Sanofi in Framingham/Massachusetts. Dr Perez-Remirez is responsible for development of protein formulations (Phase I/II clinical trials), pre-formulation research, drug delivery strategies and platform technology evaluation. He began his career at Genetics Institute (now Pfizer), joining Genzyme Sanofi in 2004. He is also the US-based Drug Device Integrator for Sanofi’s North American portfolio.
Claus Geiger, PhD MBA, is presently Global Device Project Leader and Drug Device Integrator. He started his career at Roche (Basel, Switzerland), joining Sanofi in 1997. Since then he has held various roles in the field of injectable drug delivery systems for biotherapeutics with expanding responsibility: QA/QC, Manufacturing, Supply Chain, Key Account Management of device partner companies, Global Medical Device Surveillance.
Tatyana Mezhebovsky, PhD ALM, is Senior Scientist in BioFormulations in Biopharmaceuticals Development at Sanofi in Framingham/Massachusetts and has 15 years of experience in protein formulations (from pre-formulation to commercialisation), drug delivery, biotherapeutics characterisation and the cGMP environment. She is now involved in the evaluation of the interplay of monoclonal antibody formulation and container closure effects on protein stability.
Hi Tim,
Unfortunately, with it being a historical issue I can’t provide a list; however, if you download the digital issue of the journal from the link below the article of interest can be found with the full reference list. Your article of interest starts on page 26. To zoom in closer on the pages, double click on them in the reader. Any questions, please get in touch. https://www.europeanpharmaceuticalreview.com/article/43501/issue-4-2016-digital-edition/
This website uses cookies to enable, optimise and analyse site operations, as well as to provide personalised content and allow you to connect to social media. By clicking "I agree" you consent to the use of cookies for non-essential functions and the related processing of personal data. You can adjust your cookie and associated data processing preferences at any time via our "Cookie Settings". Please view our Cookie Policy to learn more about the use of cookies on our website.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorised as ”Necessary” are stored on your browser as they are as essential for the working of basic functionalities of the website. For our other types of cookies “Advertising & Targeting”, “Analytics” and “Performance”, these help us analyse and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these different types of cookies. But opting out of some of these cookies may have an effect on your browsing experience. You can adjust the available sliders to ‘Enabled’ or ‘Disabled’, then click ‘Save and Accept’. View our Cookie Policy page.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Cookie
Description
cookielawinfo-checkbox-advertising-targeting
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertising & Targeting".
cookielawinfo-checkbox-analytics
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Analytics".
cookielawinfo-checkbox-necessary
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Performance".
PHPSESSID
This cookie is native to PHP applications. The cookie is used to store and identify a users' unique session ID for the purpose of managing user session on the website. The cookie is a session cookies and is deleted when all the browser windows are closed.
viewed_cookie_policy
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
zmember_logged
This session cookie is served by our membership/subscription system and controls whether you are able to see content which is only available to logged in users.
Performance cookies are includes cookies that deliver enhanced functionalities of the website, such as caching. These cookies do not store any personal information.
Cookie
Description
cf_ob_info
This cookie is set by Cloudflare content delivery network and, in conjunction with the cookie 'cf_use_ob', is used to determine whether it should continue serving “Always Online” until the cookie expires.
cf_use_ob
This cookie is set by Cloudflare content delivery network and is used to determine whether it should continue serving “Always Online” until the cookie expires.
free_subscription_only
This session cookie is served by our membership/subscription system and controls which types of content you are able to access.
ls_smartpush
This cookie is set by Litespeed Server and allows the server to store settings to help improve performance of the site.
one_signal_sdk_db
This cookie is set by OneSignal push notifications and is used for storing user preferences in connection with their notification permission status.
YSC
This cookie is set by Youtube and is used to track the views of embedded videos.
Analytics cookies collect information about your use of the content, and in combination with previously collected information, are used to measure, understand, and report on your usage of this website.
Cookie
Description
bcookie
This cookie is set by LinkedIn. The purpose of the cookie is to enable LinkedIn functionalities on the page.
GPS
This cookie is set by YouTube and registers a unique ID for tracking users based on their geographical location
lang
This cookie is set by LinkedIn and is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
lidc
This cookie is set by LinkedIn and used for routing.
lissc
This cookie is set by LinkedIn share Buttons and ad tags.
vuid
We embed videos from our official Vimeo channel. When you press play, Vimeo will drop third party cookies to enable the video to play and to see how long a viewer has watched the video. This cookie does not track individuals.
wow.anonymousId
This cookie is set by Spotler and tracks an anonymous visitor ID.
wow.schedule
This cookie is set by Spotler and enables it to track the Load Balance Session Queue.
wow.session
This cookie is set by Spotler to track the Internet Information Services (IIS) session state.
wow.utmvalues
This cookie is set by Spotler and stores the UTM values for the session. UTM values are specific text strings that are appended to URLs that allow Communigator to track the URLs and the UTM values when they get clicked on.
_ga
This cookie is set by Google Analytics and is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. It stores information anonymously and assign a randomly generated number to identify unique visitors.
_gat
This cookies is set by Google Universal Analytics to throttle the request rate to limit the collection of data on high traffic sites.
_gid
This cookie is set by Google Analytics and is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visited in an anonymous form.
Advertising and targeting cookies help us provide our visitors with relevant ads and marketing campaigns.
Cookie
Description
advanced_ads_browser_width
This cookie is set by Advanced Ads and measures the browser width.
advanced_ads_page_impressions
This cookie is set by Advanced Ads and measures the number of previous page impressions.
advanced_ads_pro_server_info
This cookie is set by Advanced Ads and sets geo-location, user role and user capabilities. It is used by cache busting in Advanced Ads Pro when the appropriate visitor conditions are used.
advanced_ads_pro_visitor_referrer
This cookie is set by Advanced Ads and sets the referrer URL.
bscookie
This cookie is a browser ID cookie set by LinkedIn share Buttons and ad tags.
IDE
This cookie is set by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
li_sugr
This cookie is set by LinkedIn and is used for tracking.
UserMatchHistory
This cookie is set by Linkedin and is used to track visitors on multiple websites, in order to present relevant advertisement based on the visitor's preferences.
VISITOR_INFO1_LIVE
This cookie is set by YouTube. Used to track the information of the embedded YouTube videos on a website.


 Till Bussemer, PhD, is presently Head of BioFormulation Development at Sanofi in Frankfurt, Germany, and focuses on monoclonal antibodies and large molecules. Dr Bussemer started his career at Aventis Pharmaceutical Development in 2002, where he was responsible for preformulation and formulation of solids and injectables, including depot formulations for species ranging from small molecules to biologics. Recently, Till has also become Drug Device Integrator.
Till Bussemer, PhD, is presently Head of BioFormulation Development at Sanofi in Frankfurt, Germany, and focuses on monoclonal antibodies and large molecules. Dr Bussemer started his career at Aventis Pharmaceutical Development in 2002, where he was responsible for preformulation and formulation of solids and injectables, including depot formulations for species ranging from small molecules to biologics. Recently, Till has also become Drug Device Integrator. Bernardo Perez-Ramirez, MSc PhD, is currently Senior Scientific Director of BioFormulations in the Biopharmaceuticals Development department of Sanofi in Framingham/Massachusetts. Dr Perez-Remirez is responsible for development of protein formulations (Phase I/II clinical trials), pre-formulation research, drug delivery strategies and platform technology evaluation. He began his career at Genetics Institute (now Pfizer), joining Genzyme Sanofi in 2004. He is also the US-based Drug Device Integrator for Sanofi’s North American portfolio.
Bernardo Perez-Ramirez, MSc PhD, is currently Senior Scientific Director of BioFormulations in the Biopharmaceuticals Development department of Sanofi in Framingham/Massachusetts. Dr Perez-Remirez is responsible for development of protein formulations (Phase I/II clinical trials), pre-formulation research, drug delivery strategies and platform technology evaluation. He began his career at Genetics Institute (now Pfizer), joining Genzyme Sanofi in 2004. He is also the US-based Drug Device Integrator for Sanofi’s North American portfolio. Claus Geiger, PhD MBA, is presently Global Device Project Leader and Drug Device Integrator. He started his career at Roche (Basel, Switzerland), joining Sanofi in 1997. Since then he has held various roles in the field of injectable drug delivery systems for biotherapeutics with expanding responsibility: QA/QC, Manufacturing, Supply Chain, Key Account Management of device partner companies, Global Medical Device Surveillance.
Claus Geiger, PhD MBA, is presently Global Device Project Leader and Drug Device Integrator. He started his career at Roche (Basel, Switzerland), joining Sanofi in 1997. Since then he has held various roles in the field of injectable drug delivery systems for biotherapeutics with expanding responsibility: QA/QC, Manufacturing, Supply Chain, Key Account Management of device partner companies, Global Medical Device Surveillance.





would it be possible to get the reference list for this article?
Hi Tim,
Unfortunately, with it being a historical issue I can’t provide a list; however, if you download the digital issue of the journal from the link below the article of interest can be found with the full reference list. Your article of interest starts on page 26. To zoom in closer on the pages, double click on them in the reader. Any questions, please get in touch.
https://www.europeanpharmaceuticalreview.com/article/43501/issue-4-2016-digital-edition/